There are two broad types of knee Replacement:-
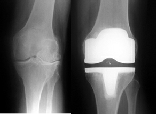
Complete :-

Where all pa rts of the joint is replaced and
rts of the joint is replaced and
Partial :-
where only one area of the joint is replaced.
Arthritis varies in severity and extent, such that some patients have arthritis that affects the entire knee joint and others have localised disease, confined to one area of the joint. In both cases, there can be painful disability which warrants surgical intervention. Your surgeon will match the implant you require to get the best outcome.
What are the advantages and disadvantages of either type?
Partial joint replacement can often be done through a smaller incision, causes less pain and quicker rehabilitation, often with a better range of movement. If it does ever wear out, revision of the replacement can be substantially easier.
Unfortunately, not all knees are suitable for partial replacements, estimates vary
between 1 in 10 and 1 in 4 arthritic knees are suitable for partial replacement.
There are also other conditions which need to be considered, for example , deficient
knee ligaments often preclude long-
Areas of the knee commonly replaced by partial joint replacement are the medial compartment
(the inside of the knee), the lateral compartment (the outside of the knee) and the
patella-
Where the arthritis is wide-
How much of the joint itself is actually replaced?
Most modern primary knee replacements aim to replace only the damaged surface of the knee joint, retaining as much of the native bone. By accurately cutting the bone ends to fit, the implant can be placed in such a way to reform the natural shape of the knee, but with a smooth and painless surface.
How are the components of a knee replacement fixed to the patients bone?
There are several ways this can be achieved, most commonly by using cement. The cement is however a specially designed material (polymethyl methacrylate) which is mixed at the time of implantation, and used as a grout to fix the component. It sets in about 10 minutes to give solid fixation immediately. The cement can be mixed with antibiotics to provide additional protection against infection. The main disadvantage of cement is that it adds time to the length of the procedure. Also it is believed that particles that separate from the cement mantle can cause accelerated wear of the implant.
Most Knee implants have an "un-
How are the joints lubricated?
Between the metal components, there is a layer of very strong plastic (polyethylene) which is very smooth and slippery. Together with the natural lubricant of the knee, there is very little friction and the joint glides smoothly without catching.


| Personal Details |
| Orthopaedic Surgical Team |
| Personal Results |
| Background Information |
| Sports Injury |
| Arthritis |
| Surgical Guides |
| Pre Operative Guides |
| Post Operative Guides |
| Alexandra Hospital |